Arthroscopic shoulder surgery by a shoulder arthroscopy surgeon in Ahmedabad treats rotator cuff tears and shoulder instability through two or three tiny incisions, with no large open wound and no prolonged hospital stay. Precise repair under direct camera vision with advanced shoulder scope surgery. Back to daily life in weeks, sport in months.
Our specialist will call you within 2 hours
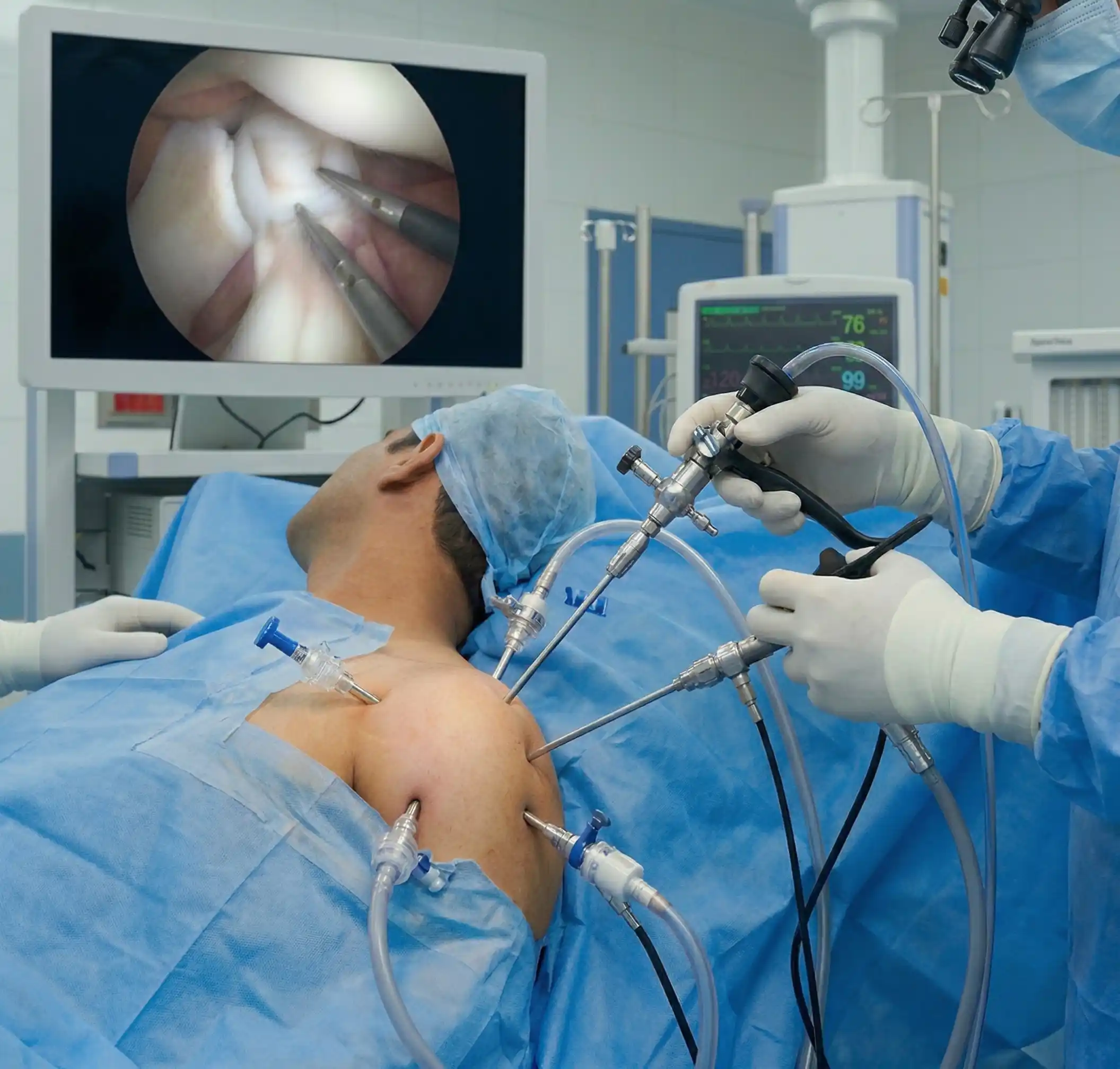
Shoulder arthroscopy is a minimally invasive surgical procedure in which a thin camera — the arthroscope — is inserted into the shoulder joint through a small incision approximately 5mm in size. The camera transmits a magnified, high-definition view of the structures inside the shoulder — rotator cuff tendons, labrum, biceps tendon, bursa and joint cartilage — onto a screen, allowing the surgeon to diagnose and treat a wide range of shoulder conditions without the large incisions, extended hospital stay and prolonged recovery of open shoulder surgery.
At Trayam Hospital, shoulder arthroscopy is performed as a day-care procedure under general anaesthesia — most patients are discharged the same day. Through two or three small portals, the surgeon introduces instruments alongside the camera to repair torn tendons, reattach the labrum, remove inflamed tissue or address instability — all under direct vision with precision that open surgery cannot match. The procedure is both diagnostic and therapeutic: confirming exactly what is damaged and repairing it in the same session.
If you're experiencing any of these symptoms, a consultation with a shoulder arthroscopy surgeon is recommended
Pain when raising the arm between 60 and 120 degrees — the classic painful arc of rotator cuff disease. Caused by the torn or impinged tendon being compressed against the acromion during mid-range elevation. The pain often eases above 120 degrees, then returns when lowering.
Inability to sleep on the affected shoulder, or being woken by pain when rolling onto it. Night pain is a hallmark of significant rotator cuff pathology — the torn tendon loses its resting tension and the shoulder is painful in any position without the upright muscle activity that partially splints it during the day.
Weakness when lifting, pushing or reaching — difficulty with overhead tasks, carrying shopping or lifting objects away from the body. Rotator cuff tears cause a measurable reduction in shoulder strength that physiotherapy cannot fully restore when the structural tear is significant.
The shoulder has dislocated once or multiple times — the ball (humeral head) coming completely out of the socket. A first-time dislocation in a young active patient carries a 70–90% risk of recurrence without surgical stabilisation. Recurrent dislocation is almost always an indication for arthroscopic Bankart repair.
A feeling that the shoulder is about to dislocate during certain movements — particularly arm elevation and external rotation (the "throwing position"). This apprehension is caused by a labral or ligament deficiency that makes the shoulder structurally unstable even without a full dislocation.
MRI confirming a partial or full-thickness rotator cuff tear — supraspinatus, infraspinatus or subscapularis. Tear size, tissue quality and symptom duration determine whether surgical repair, physiotherapy or augmented repair is the right approach. Large tears treated late become irreparable — early assessment matters.
Persistent shoulder pain — rotator cuff-type or instability-type — that has not improved adequately after 3–6 months of structured physiotherapy. When conservative management has failed to resolve a structurally based problem, arthroscopic assessment and treatment is the logical next step.
Shoulder injury during sport — a throwing injury, tackle, collision or fall onto an outstretched arm — causing immediate pain, instability or weakness. Sports shoulder injuries frequently involve the rotator cuff, labrum or both. Continuing to play through significant structural damage accelerates tear progression.
Athletes, working professionals and patients of all ages choose Trayam Hospital for shoulder arthroscopy

Senior Consultant — Shoulder, Elbow & Sports Surgery, Trayam Hospital
Dr. Parth Patel is an experienced shoulder arthroscopy specialist with fellowship training in shoulder and upper limb surgery. With over 2,000 arthroscopic shoulder procedures performed — including complex rotator cuff repairs, Bankart stabilisations and revision shoulder surgery — Dr. Parth Patel combines surgical precision with a deep understanding of what patients need most: not just pain relief, but full, confident return to the activities and sports they love.
Shoulder arthroscopy at Trayam addresses the two most common surgical shoulder conditions — rotator cuff tears and shoulder instability — with the full range of arthroscopic techniques
Day-care procedure complete. Arm in a sling. Discharged same day or next morning. Ice, pain medication and sling instructions provided. Gentle finger, wrist and elbow movement encouraged from day 1.
Sling worn continuously (rotator cuff repair: 4–6 weeks; Bankart repair: 3–4 weeks). Passive range-of-motion exercises begin at physiotherapy. Portal wounds healing — reviewed at 10–14 days. Desk work possible from week 2–3 with sling.
Sling weaned. Active-assisted range-of-motion exercises progressing. Swelling and stiffness reducing. Physiotherapy attending regularly — range of motion and early strengthening.
Active range of motion restored for most patients. Rotator cuff strengthening programme underway. Bankart patients: shoulder confidence returning, contact avoided.
Strengthening near completion. Return to light recreational sport. Rotator cuff repair patients: overhead activity progressing. Full strength testing at physiotherapy assessment.
Return to full sport and unrestricted activity for most patients — rotator cuff repair and Bankart repair. Final outpatient review with assessment of strength, stability and range of motion. Annual review not required unless symptoms recur.
A few of the most common mismanagement patterns in shoulder surgery in India are: managing a significant rotator cuff tear with repeated steroid injections until the tear becomes irreparable, and treating recurrent shoulder dislocation with physiotherapy alone when surgical stabilisation is the only reliable solution. In both cases, delay worsens the outcome — and in rotator cuff disease, extended delay can convert a repairable tear into an irreparable one.
Fully itemised estimate covering procedure, anaesthesia, day-care stay, implants (suture anchors specified), physiotherapy and follow-up — in writing before you book. No surprises after surgery.
We do not recommend arthroscopy for shoulder conditions that will respond to structured physiotherapy. We do recommend it when structural pathology — a repairable tear or correctable instability — will not resolve without surgery. Honest assessment, every time.
Shoulder arthroscopy, rotator cuff repair and Bankart stabilisation are covered under most major Indian health insurance policies. Our insurance desk manages pre-authorisation and cashless hospitalisation for all shoulder procedures.
Shoulder pain, weakness or instability? Get an honest assessment — not another injection.
Confidential · No Obligation · Reply in 2 Hours
Shoulder arthroscopy inserts a thin camera into the shoulder through a 5mm incision. The surgeon views the joint on a screen and repairs damaged structures through two or three additional small portals. Performed under general anaesthesia — usually day care.
Rotator cuff repair: 60–90 minutes. Bankart repair: 45–75 minutes. Remplissage with Bankart: 75–90 minutes. Diagnostic arthroscopy: 30–45 minutes.
Rotator cuff repair: sling for 4–6 weeks to protect the repair while the tendon heals to bone. Bankart repair: sling for 3–4 weeks. The sling duration reflects the healing time required — not the severity of the procedure.
Desk work: 2–4 weeks with sling. Light manual work: 3–4 months. Heavy manual work and overhead labour: 5–6 months. Return-to-work timing is individualised based on procedure and job demands.
Non-contact recreational sport: 4–5 months. Overhead sport (cricket, tennis, swimming): 5–6 months. Contact sport and collision sports: 6 months after Bankart repair. Return to play requires sign-off from both the surgeon and physiotherapist.
In correctly selected patients without significant bone loss, arthroscopic Bankart repair achieves over 90% stability at medium-term follow-up. Patients with significant glenoid bone loss (over 20–25%) may require additional bone grafting procedures (Latarjet) for equivalent stability.
Shoulder arthroscopy is a safe procedure. Risks include: infection (under 1%), stiffness, failure of repair requiring revision, and — rarely — nerve or vessel injury. Stiffness is more common after rotator cuff repair (5–10%) and is managed with physiotherapy.
Yes — rotator cuff repair and Bankart stabilisation are covered by most major Indian health insurance policies and PMJAY. Our insurance desk manages pre-authorisation and cashless hospitalisation.
Talk to our shoulder specialist today — bring your MRI if you have one, or we arrange it. Book a consultation, no obligation.
