Sudden leg weakness, numbness or loss of bladder/bowel control? These are emergency spinal cord symptoms — seek immediate care now.
The same surgical results as open spine surgery, through incisions smaller than 2cm by a minimally invasive spine surgeon in Ahmedabad. Less muscle damage, less blood loss, and most patients walk the same day. Same-day and next-morning consultations available.
Tell us your symptoms — we'll respond within 2 hours
100% confidential & no obligation
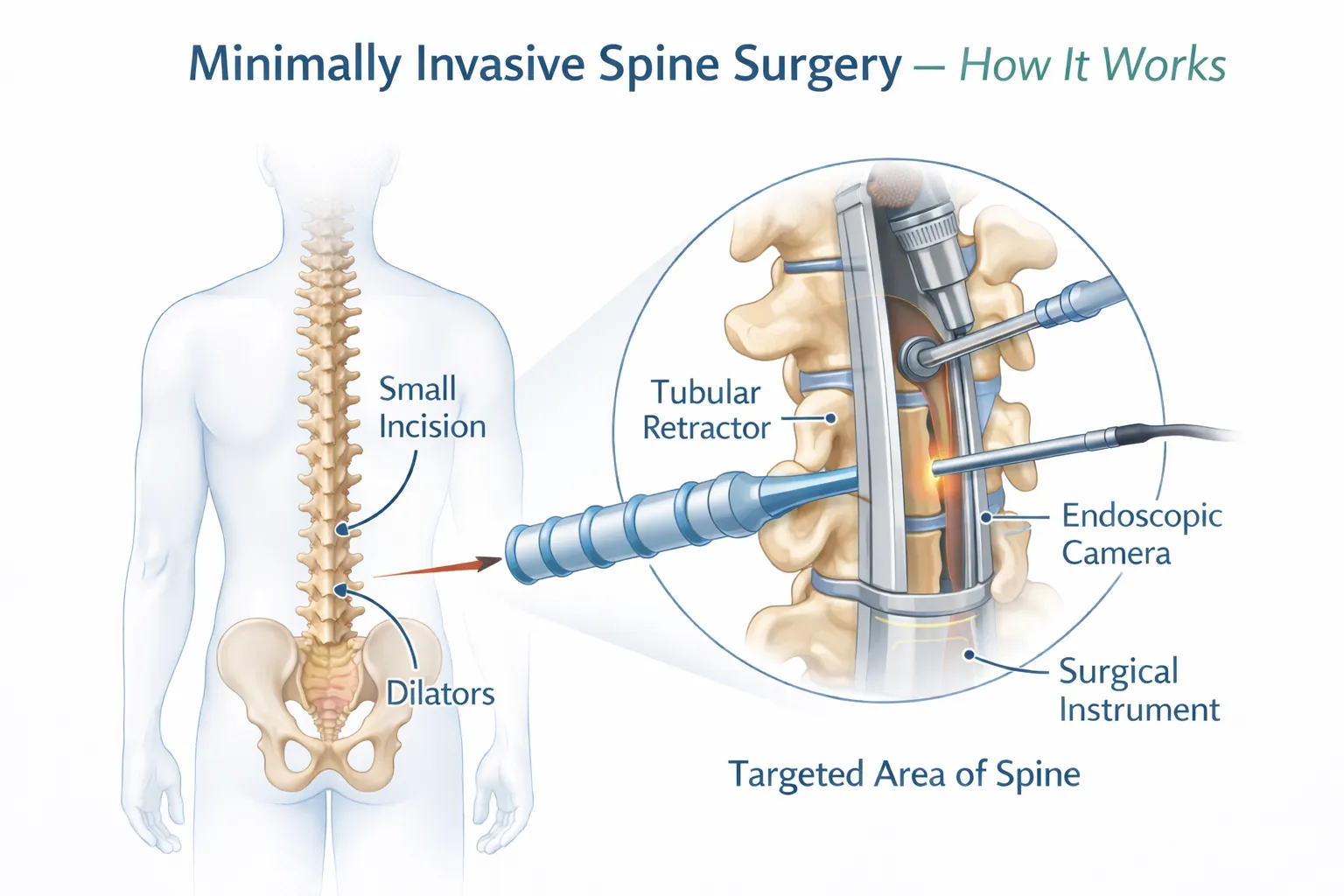
Minimally invasive spine surgery uses tiny keyhole incisions — typically under 2cm — combined with specialised tubular retractors, surgical microscopes or endoscopes to treat the exact same spinal conditions as traditional open surgery. The critical difference: muscles are gently dilated rather than cut and retracted, causing less tissue damage dramatically.
The result is significantly reduced post-operative pain, less blood loss, a lower risk of infection, and a recovery measured in days rather than weeks or months. At Trayam Hospital, minimally invasive spine surgery is the standard approach for eligible spine conditions — not a premium add-on.
A tubular retractor dilates a pathway to the spine through a 1.5–2cm incision. A surgical microscope provides magnified, illuminated visualisation to remove disc material or decompress nerves with pinpoint precision.
Gold StandardPercutaneous pedicle screws and a cage are inserted through tiny stab incisions to fuse an unstable spinal segment. Avoids the extensive muscle stripping of open fusion surgery, dramatically reducing pain and recovery time.
Minimally Invasive FusionA balloon is inserted into a fractured vertebra to restore height, then filled with bone cement — all through a needle-sized access. Immediate pain relief for vertebral compression fractures with no open incision required.
Fracture Treatment
Fusion approached from the patient's side through a tiny flank incision, avoiding back muscles entirely. Allows insertion of a large fusion cage to restore disc height and spinal alignment with minimal approach-related morbidity.
Advanced TechniqueRed symptoms are neurological emergencies requiring immediate care. Other symptoms warrant urgent specialist assessment — early treatment prevents permanent nerve damage.
Sharp, burning or shooting pain running from the lower back through the buttock and down the leg — classic nerve compression
Loss of bladder or bowel control, saddle numbness around groin — cauda equina syndrome is a surgical emergency requiring immediate surgery
Chronic lower back or neck pain unresponsive to 6+ weeks of physiotherapy and medication — may indicate structural pathology
Difficulty lifting the foot while walking, leg giving way or progressive weakness — indicates significant nerve or cord compression requiring urgent assessment
Pain, tingling or weakness radiating from the neck into the shoulder, arm or fingers — cervical disc herniation or cervical spondylosis
Pins and needles, burning or numbness in the hands, arms, legs or feet — indicates nerve compression that requires investigation
Leg pain, cramping or heaviness that appears after walking short distances and is relieved by bending forward — hallmark of lumbar spinal stenosis
Back or neck pain that has not responded to 6–12 weeks of physiotherapy, medication and rest — time to consider surgical evaluation
From simple microdiscectomy to complex minimally invasive fusion — the right procedure is chosen based on your exact diagnosis, spinal level and anatomy.
Hundreds of patients have regained their active lives through minimally invasive spine surgery at Trayam Hospital with proven clinical outcomes

Senior Consultant Spine Surgeon — Minimally Invasive & Endoscopic Spine Surgery
Dr. Parth Patel is a highly experienced spine surgeon specialising exclusively in minimally invasive and endoscopic techniques. With over 1,000 spine procedures performed — including MIS-TLIF, microdiscectomy, XLIF and kyphoplasty — the focus is always on achieving maximum clinical benefit with minimum surgical trauma.
Spine surgery is one of the most over-prescribed specialties globally. Many patients are offered unnecessary surgery, or open procedures when minimally invasive options would achieve the same result with far less risk and recovery time.
We review your MRI, CT and clinical examination in full before suggesting any procedure. Imaging findings must correlate with your symptoms — we never treat a scan alone.
Unless there is a neurological emergency, we trial physiotherapy, pain management and injection therapy before recommending surgery. Many patients find lasting relief without any procedure.
Every surgical patient receives a personalised physiotherapy programme starting day one post-surgery. Spine surgery without rehabilitation is incomplete care — we never discharge without a clear recovery roadmap.
Get an honest second opinion or first consultation — we'll tell you honestly whether you need surgery, which type, and whether minimally invasive is suitable for your specific condition.
Minimally invasive surgery gives you a head start on recovery — but what you do after surgery determines your final outcome. Here's how to get the best results.
Minimally invasive spine surgery (MISS) uses tiny keyhole incisions — usually under 2cm — combined with specialised tubular retractors and surgical microscopes or endoscopes. The key difference from open surgery is that muscles are gently dilated rather than cut and retracted, causing dramatically less tissue damage. The surgical goals — disc removal, nerve decompression, spinal fusion — are identical, but recovery is measured in days rather than months.
Most patients with lumbar disc herniation, spinal stenosis, spondylolisthesis or single to multi-level degenerative disease are candidates. Suitability depends on your specific diagnosis, spinal anatomy, degree of deformity and overall health. Obesity, severe deformity or multilevel complex disease may necessitate hybrid or open approaches. Our spine surgeon will review your MRI and clinical findings to advise precisely.
Recovery is significantly faster than open surgery. Most patients walk the same day, are discharged in 24–48 hours, and return to desk work in 2–4 weeks. Physical labour resumes at 8–12 weeks. For fusion procedures, bony healing occurs over 3–6 months, though most functional activities resume much sooner. A structured physiotherapy programme is essential to maximise and maintain the surgical result.
Most back pain resolves with 6–12 weeks of physiotherapy, medication and activity modification. Surgery is considered when: pain is severe and unresponsive to structured conservative treatment; there is progressive neurological deficit (weakness, numbness, foot drop); cauda equina syndrome is suspected (bladder or bowel involvement — this is an emergency); or imaging confirms a structural abnormality directly causing the symptoms. Our surgeon will guide you honestly.
Yes — multiple clinical studies confirm that minimally invasive techniques achieve equivalent or superior clinical outcomes to open surgery for appropriate indications, with significantly lower complication rates, less blood loss, reduced infection risk and dramatically faster recovery. The surgical goals — nerve decompression, disc removal, spinal stabilisation — are achieved with the same precision through smaller access.
Cauda equina syndrome occurs when a large disc herniation or other lesion severely compresses the nerve bundle at the base of the spinal cord. Symptoms include bilateral leg weakness or numbness, saddle anaesthesia (numbness around the groin and inner thighs), and loss of bladder or bowel control. This is a surgical emergency — decompression surgery within hours of onset is critical to prevent permanent paralysis and incontinence. If you experience these symptoms, go to emergency immediately.
Absolutely — physiotherapy is as important as the surgery itself. A structured rehabilitation programme starting within 48 hours of minimally invasive spine surgery includes early mobilisation, posture training, core strengthening, neural mobilisation and a graded return-to-activity plan. Patients who complete their rehabilitation programme consistently achieve better, more durable outcomes than those who do not. Our physiotherapy team in Ahmedabad is embedded within the spine unit and provides an individualised programme for every patient.
Yes — minimally invasive spine surgery including microdiscectomy, MIS-TLIF fusion, laminectomy and kyphoplasty is covered by most health insurance policies in India. Trayam Hospital is empanelled with all major insurers with cashless facility. Our insurance desk manages pre-authorisation and claims support from the day of your first consultation.
Microscopic (tubular) spine surgery uses a surgical microscope for magnified vision through a small tubular retractor — the most widely used MISS technique. Endoscopic spine surgery passes a tiny camera through a needle-sized portal and uses continuous saline irrigation to maintain working space, requiring no incision larger than a few millimetres. Endoscopic is the most minimally invasive approach and is ideal for soft disc herniations and foraminal stenosis. Our surgeon will advise which approach is most appropriate for your anatomy and diagnosis.
Same-day consultations available. Honest advice — we'll guide you to the right treatment, not the most expensive one.
