Completely unable to pass urine? Acute urinary retention from BPH obstruction is a urological emergency — call immediately, do not wait.
From early BPH managed with medication to severe obstruction treated with gold-standard laser HoLEP — our expert urologist provides the right care for your prostate at every stage. Same-day consultations available for TURP surgery.
Tell us your symptoms — we'll respond within 2 hours
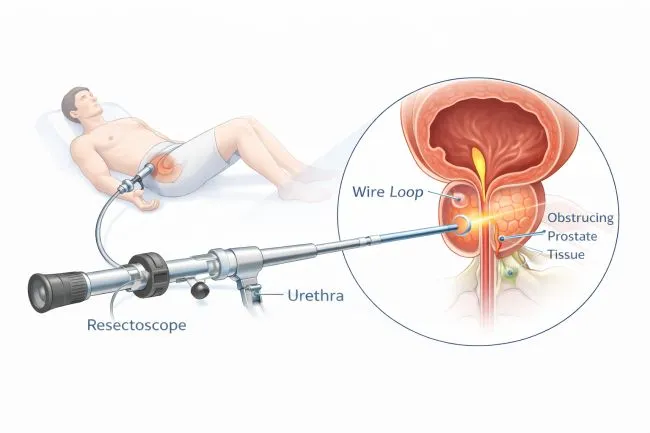
TURP — Transurethral Resection of the Prostate — removes the prostate tissue blocking urine flow entirely through the urethra. A resectoscope instrument is passed through the urethra to the prostate, where a wire loop uses electrical energy to cut away the obstructing tissue. There is no skin incision whatsoever — the entire procedure is endoscopic.
TURP has a 50-year proven track record as the surgical gold standard for BPH. Modern bipolar TURP uses saline irrigation instead of glycine — completely eliminating TURP syndrome, a dangerous fluid absorption complication of older monopolar technique. Most patients notice a dramatic improvement in urine stream from the day the catheter is removed.
TURP is not the first step for BPH — medication always comes first. But when medication fails or complications arise, TURP delivers reliable, lasting relief. These are the four main indications.
Moderate-to-severe BPH persisting despite a 3–6 month trial of alpha-blockers and 5-ARIs. TURP is the most effective surgical option for prostate glands of 30–80g when medication alone is no longer adequate.
Most CommonComplete inability to pass urine requiring emergency catheterisation. Once stabilised, TURP is planned as the definitive treatment to remove the obstruction and prevent further retention episodes.
EmergencyRecurrent or persistent blood in urine from highly vascular enlarged prostate blood vessels. TURP removes the bleeding source — the vascular prostatic tissue — resolving haematuria in over 95% of cases.
Haematuria ControlResidual urine from chronic BPH obstruction creates a breeding ground for bacteria. TURP resolves the underlying obstruction — stopping the cycle of recurrent infections and preventing progressive bladder or kidney damage.
Infection PreventionThese obstructive and irritative voiding symptoms — caused by BPH squeezing the urethra — respond dramatically to TURP when medication alone is no longer sufficient.
Suddenly unable to pass any urine at all — emergency catheterisation needed immediately. Call us now.
Consistently slow, thin or hesitant stream — worsening progressively over months or years. The hallmark symptom of BPH obstruction.
Waking 3–6 times per night to urinate — severely disrupting sleep quality and daytime energy. A leading quality-of-life complaint in BPH.
Sudden intense urge to urinate every 30–60 minutes, unable to delay. Overactive bladder secondary to BPH outflow obstruction.
Needing to push, strain or wait 30–60 seconds before urination starts — the prostate squeezing the urethra resists flow initiation.
Bladder never fully empties — residual urine causes infection risk and the sensation of needing to go again soon after finishing.
Pink or red urine from vascular enlarged prostate blood vessels. Painless intermittent haematuria from BPH is a recognised TURP indication.
3–6 months of alpha-blockers and 5-ARIs with inadequate relief — a clear indication that TURP or HoLEP surgical treatment is the right next step.
Not every enlarged prostate needs surgery. We always start with the simplest effective option — and only recommend TURP when it is genuinely the right next step for your specific prostate and circumstances.
Our TURP programme combines bipolar technology, honest surgical decision-making and 24/7 emergency access — the right patient gets the right procedure at the right time.

Senior Consultant Urologist & Prostate Surgery Specialist — Trayam Hospital
Dr. Renish Patel has performed over 5,000 TURP procedures — including complex cases in older patients with cardiovascular comorbidities and patients on anticoagulant therapy. The surgical philosophy is straightforward: complete a proper medication trial first, use the safest modern technique (bipolar TURP), and recommend HoLEP honestly when it is the better option for the patient's specific prostate size.
TURP is an excellent, proven procedure — but it should only be recommended when medication has genuinely failed, or when a clear complication makes surgery necessary. Here are the red flags patients often encounter.
Uroflowmetry, post-void residual scan and IPSS score are completed at every consultation. Surgical decisions are based on objective data — not just reported symptoms alone.
For prostates under 80g, bipolar TURP is excellent. For larger glands or patients wanting the lowest re-treatment rate, we recommend HoLEP — and explain the reasons clearly so you can make an informed decision.
All TURP procedures at Trayam use bipolar technology with saline irrigation. We do not perform monopolar TURP. Modern, safer technique as the non-negotiable standard of care.
Have BPH symptoms? Uncertain whether you need TURP?
Bring your PSA and uroflowmetry if available — or we start fresh. We’ll tell you honestly whether medication can still help, or whether TURP is the right next step.
Confidential · No Obligation · Reply in 2 Hours
TURP recovery is faster than open surgery — most patients are home within 2–3 days with significant improvement in urine flow apparent from the day the catheter is removed.
Yes — TURP remains highly effective for moderate BPH with prostate size 30–80g and continues to be performed widely globally. HoLEP has advantages for large prostates over 80g and lower re-treatment rates. Our urologist recommends the most appropriate procedure based on your specific prostate size, overall health and priorities.
Retrograde ejaculation — where semen goes into the bladder rather than outward — occurs in 60–90% of TURP patients. This does not affect sexual pleasure, orgasm or erection quality. Permanent erectile dysfunction from modern bipolar TURP is rare (under 5%). We discuss all sexual function outcomes honestly before surgery so you can make a fully informed decision.
TURP typically takes 30–90 minutes under spinal anaesthesia. A urethral catheter remains in place for 24–48 hours post-procedure. Most patients are discharged on day 2–3 once passing urine comfortably with good flow and minimal bleeding.
Bipolar TURP uses saline irrigation instead of glycine, eliminating the risk of TURP syndrome — a dangerous fluid absorption complication of traditional monopolar TURP causing dilutional hyponatraemia. Bipolar TURP is now the standard at well-equipped centres and is significantly safer, particularly for older patients and longer procedures.
Most patients notice significantly improved urine stream from the moment the catheter is removed on day 2–3. Some temporary urgency and frequency for 2–4 weeks as the bladder adjusts is normal and resolves with pelvic floor exercises. Maximum flow improvement is achieved by 6–8 weeks post-operatively.
TURP provides durable long-term results — 85–90% of patients maintain significant symptom improvement at 5 years. Approximately 10–15% may require a second procedure over 10–10 years as remaining prostate tissue continues to grow with age. HoLEP has a slightly lower re-treatment rate due to more complete enucleation.
Yes — TURP under spinal anaesthesia is well-tolerated by older patients including those with cardiovascular or respiratory comorbidities. Spinal anaesthesia avoids general anaesthesia risks. Pre-operative cardiac and anaesthesia assessment and optimisation is thorough for every patient. Bipolar TURP further reduces risk by eliminating fluid absorption complications.
Pre-operative workup includes: PSA blood test, uroflowmetry, post-void residual scan, prostate ultrasound, urine culture, full blood count, renal function tests, ECG and anaesthesia fitness assessment. We complete as many investigations as possible at the time of the initial consultation.
Yes — TURP is covered by virtually all Indian health insurance policies including Star Health, HDFC ERGO, United India, New India Assurance, Bajaj Allianz and all government schemes. Trayam Hospital is empanelled with all major insurers. Our team handles cashless pre-authorisation, paperwork and full claim support from day one.
TURP is highly suitable for prostates of 30–80g when HoLEP is not available or not preferred. HoLEP offers advantages for large prostates over 80g, patients on anticoagulants and those prioritising the lowest re-treatment rate over the long term. Our urologist provides a specific honest recommendation based on your prostate size, flow data and individual priorities.
Bring your PSA and uroflowmetry — or we start fresh. Honest advice on whether medication can still work or TURP is the right next step.



